“Imagine being bombarded day & night by volleys of acoustic artillery, much of it low frequency and infrasonic” (Dr. Pierpont)
Jul 2, 2014
.
Editor’s note: The following is a letter Dr. Pierpont wrote to a group in Turkey that’s trying to keep wind turbines out of its community. (Click here for a PDF.) We are told the wind developer has been ordered by a court to stop building the turbines. Being Turkey, the developer has brazenly ignored the court order — and is proceeding full steam ahead. (So much for the “rule of law.”)
.
To: Ms. Kabadayi-Whiting, Cesme, Turkey
From: Nina Pierpont, MD, PhD
Regarding: The proper siting of wind turbines
Date: June 30, 2014
.
I write to you at the request of Madeleine Kura, who tells me the lovely, seaside town of Cesme is about to get half a dozen 3 MW industrial wind turbines built on the edge of town, a mere 500 m from people’s homes. (I’m told that at least one of the turbines will be 300 m from a school.) Furthermore, all this construction will be in hilly terrain.

Let me explain, clinically, why this is a bad idea. In 2009 I published what was then the definitive study of health effects caused by wind turbine infrasound on people living within 2 km of industrial turbines. The book, “Wind Turbine Syndrome: A Report on a Natural Experiment” (K-Selected Books), included 60 pages of raw data in the form of case histories (using case cross-over studies), demonstrating that living in proximity to wind turbines dys-regulates the inner ear vestibular organs controlling balance, position, and spatial awareness. Effectively, sufferers experience symptoms of sea-sickness, along with several related pathologies.
It turns out all this has been well known since the 1980s, when the US Department of Energy commissioned a report on wind turbine health effects — the report subsequently published by physicist Dr. N D Kelley and his colleagues at the Solar Research Institute in Golden, Colorado, bearing the title, “A Methodology for Assessment of Wind Turbine Noise Generation,” Transactions of the American Society of Mechanical Engineers, v. 104 (May 1982), pp. 112-120.
In this paper we have presented evidence to support the hypothesis that one of the major causal agents responsible for the annoyance of nearby residents by wind turbine noise is the excitation of highly resonant structural and air volume modes by the coherent, low-frequency sound radiated by large wind turbines.
Further, there is evidence that the strong resonances found in the acoustic pressure field within rooms [in people’s homes] . . . indicates a coupling of sub-audible energy [infrasound] to human body resonances at 5, 12, and 17-25 Hz, resulting in a sensation of whole-body vibration (p. 120).
I discovered the same thing in my research. What Kelly et al. refer to as a “sensation of whole-body vibration,” I refer to as Visceral Vibratory Vestibular Disturbance (VVVD): “The internal quivering, vibration, or pulsation and the associated complex of agitation, anxiety, alarm, irritability, tachycardia, nausea, and sleep disturbance together make up what I refer to as Visceral Vibratory Vestibular Disturbance (VVVD)” (Wind Turbine Syndrome, p. 59).

Five years later, Dr. Kelley gave a follow-up paper at the Windpower ’87 Conference & Exposition in San Francisco, titled “A Proposed Metric for Assessing the Potential of Community Annoyance from Wind Turbine Low-Frequency Noise Emissions.” Just so you understand the terminology, “emissions” means “noise & vibration.” And the term “low frequency” includes infrasound. And the antiseptic phrase “community annoyance” is code for Wind Turbine Syndrome — except the name had not been coined in1987. (I created it decades later.) Kelley’s research once again had been funded by the US Department of Energy, Contract No. DE-AC02-83CH10093.
We electronically simulated three interior environments resulting from low-frequency acoustical loads radiated from both individual turbines and groups of upwind and downwind turbines. . . .
Experience with wind turbines has shown that it is possible . . . for low-frequency acoustic noise radiated from the turbine rotor to interact with residential structures of nearby communities and annoy the occupants. . . .
The modern wind turbine radiates its peak sound power (energy) in the very low frequency range, typically between 1 and 10 Hz [i.e., infrasound]. . . .
Our experience with the low-frequency noise emissions from a single, 2 MW MOD-1 wind turbine demonstrated that . . . it was possible to cause annoyance within homes in the surrounding community with relatively low levels of LF-range [low frequency range] acoustic noise. An extensive investigation of the MOD-1 situation revealed that this annoyance was the result of a coupling of the turbine’s impulsive low-frequency acoustic energy into the structures of some of the surrounding homes. This often created an annoyance environment that was frequently confined to within the home itself (p. 1, emphasis in original).
I am attaching a copy of Kelley’s 1987 paper.
Besides my research, which pretty much duplicates Kelley’s, there is the work of Dr. Alec Salt, Professor of Otolaryngology in the School of Medicine at Washington University (St. Louis, Missouri), where he is director of the Cochlear Fluids Research Laboratory. Professor Salt is a highly respected neuro-physiologist specializing in inner ear disorders and in particular the mysteries of the cochlea.

Prof. Salt’s research dovetails with mine and with Dr. Kelley’s. For many years, acousticians and noise engineers have vigorously maintained that “if you can’t hear it, it can’t hurt you.” That is to say in the case of wind turbines, “If you can’t hear the low-frequency noise in the infrasound range, it can’t hurt you.” (lnfrasound, by definition, is noise below the hearing threshold, typically pegged at 20 Hz and lower. People feel infrasound in various parts of the body, though typically they cannot hear it.) In any case, Professor Salt and his colleagues have demonstrated conclusively, definitively, that infrasound does in fact disturb the very fine hair cells of the cochlea.
With this discovery, one of the main arguments advanced by the wind energy industry — namely, that wind turbine infrasound was too low to be harmful to people, since they could not hear it — was demolished. Prof. Salt has proven that, “If you can’t hear it, it can still harm you.”
This past winter, Professor Salt and his colleague, Professor Lichtenhan, published “How Does Wind Turbine Noise Affect People?” Acoustics Today, v. 10 (Winter 2014), pp. 20-28. The following is a lengthy excerpt:
The essence of the current debate is that on one hand you have the well-funded wind industry (1) advocating that infrasound be ignored because the measured levels are below the threshold of human hearing, allowing noise levels to be adequately documented through A-weighted sound measurements; (2) dismissing the possibility that any variants of wind turbine syndrome exist (Pierpont 2009) even when physicians (e.g., Steven D. Rauch, M.D. at Harvard Medical School) cannot otherwise explain some patients’ symptoms; and (3) arguing that it is unnecessary to separate wind turbines and homes based on prevailing sound levels.
On the other hand, you have many people who claim to be so distressed by the effects of wind turbine noise that they cannot tolerate living in their homes. Some move away, either at financial loss or bought-out by the turbine operators. Others live with the discomfort, often requiring medical therapies to deal with their symptoms. Some, even members of the same family, may be unaffected. Below is a description of the disturbance experienced by a woman in Europe we received a few weeks ago as part of an unsolicited e-mail.
From the moment that the turbines began working, I experienced vertigo-like symptoms on an ongoing basis. In many respects, what I am experiencing now is actually worse than the ‘dizziness’ I have previously experienced, as the associated nausea is much more intense. For me the pulsating, humming, noise that the turbines emit is the predominant sound that I hear and that really seems to affect me.
While the Chief Scientist [the person who came to take sound measurements in her house] undertaking the measurement informed me that he was aware of the low frequency hum the turbines produced (he lives close to a wind farm himself, and had recorded the humming noise levels indoors in his own home) he advised that I could tune this noise out and that any adverse symptoms I was experiencing were simply psychosomatic. . . .
Given the knowledge that the ear responds to low frequency sounds and infrasound, we knew that comparisons with benign sources were invalid and the logic to A-weight sound measurements was deeply flawed scientifically. . . .
From this understanding we conclude that very low frequency sounds and infrasound, at levels well below those that are heard, readily stimulate the cochlea. Low frequency sounds and infrasound from wind turbines can therefore stimulate the ear at levels well below those that are heard. . . .
No one has ever evaluated whether tympanostomy tubes alleviate the symptoms of those living near wind turbines. From the patient’s perspective, this may be preferable to moving out of their homes or using medical treatments for vertigo, nausea, and/or sleep disturbance. The results of such treatment, whether positive, negative, would likely have considerable scientific influence on the wind turbine noise debate….
Another concern that must be dealt with is the development of wind turbine noise measurements that have clinical relevance. The use of A-weighting must be reassessed as it is based on insensitive, Inner Hair Cell (IHC)-mediated hearing and grossly misrepresents inner ear stimulation generated by the noise. In the scientific domain, A-weighting sound measurements would be unacceptable when many elements of the ear exhibit a higher sensitivity than hearing. The wind industry should be held to the same high standards. Full-spectrum monitoring, which has been adopted in some reports, is essential. . . .
Given the present evidence, it seems risky at best to continue the current gamble that infrasound stimulation of the ear stays confined to the ear and has no other effects on the body. For this to be true, all the mechanisms we have outlined (low frequency-induced amplitude modulation, low frequency sound-induced endolymph volume changes, infrasound stimulation of type II afferent nerves, infrasound exacerbation of noise-induced damage and direct infrasound stimulation of vestibular organs) would have to be insignificant. We know this is highly unlikely and we anticipate novel findings in the coming years that will influence the debate.
I suspect you are beginning to get a clear picture of the problem — and why I’m writing to you.
The typical symptoms of what is now known worldwide as Wind Turbine Syndrome are: sleep disturbance, headache, tinnitus (ringing or buzzing in the ears), ear pressure, dizziness (a general term that includes vertigo, light-headedness, sensation of almost fainting, etc.). nausea, visual blurring, tachycardia (rapid heart rate), irritability, problems with concentration and memory, and panic episodes associated with sensations of internal pulsation or quivering which arise when awake or asleep.
Does everybody living near wind turbines experience Wind Turbine Syndrome? By no means! What I discovered is that people with (a) motion sensitivity, (b) migraine disorder, (c) the elderly (50 years and older), (d) inner ear damage, and (e) autistic children and adults — all these are at statistically significant high risk.
The solution is simple: industrial wind turbines must be set back, well away from people’s homes, schools, places of work, and anywhere else people regularly congregate. In my 2009 report, I recommended a minimum setback of 2 km in level terrain. Studies done around the world since then have persuaded me that 2 km is not sufficient, especially in hilly or mountainous terrain — as with Cesme. In Cesme’s case, setbacks should be more on the order of 5 km or greater.
Hence my alarm when notified by Ms. Kura that Cesme is considering 500 m (or less) setbacks. This is wholly inadequate. I guarantee that, unless the setbacks are increased substantially, there will be numerous victims of Wind Turbine Syndrome.

There’s more. Dr. Salt referred to Dr. Steven Rauch, above. Dr. Rauch, a physician, is the Medical Director of Harvard Medical School’s renowned Clinical Balance and Vestibular Center, part of the Massachusetts Eye & Ear Infirmary. Dr. Rauch was recently interviewed by The New Republic:
Dr. Steven Rauch, an otologist at the Massachusetts Eye and Ear Infirmary and a professor at Harvard Medical School, believes WTS [Wind Turbine Syndrome] is real. Patients who have come to him to discuss WTS suffer from a “very consistent” collection of symptoms, he says. Rauch compares WTS to migraines, adding that people who suffer from migraines are among the most susceptible to turbines. There’s no existing test for either condition but “Nobody questions whether or not migraine is real.”
“The patients deserve the benefit of the doubt,” Rauch says. “It’s clear from the documents that come out of the industry that they’re trying very hard to suppress the notion of WTS and they’ve done it in a way that [involves] a lot of blaming the victim” (“Big Wind Is Better Than Big Oil, But Just as Bad at P.R.,” by Alex Halperin in The New Republic, June 16, 2014).
Dr. Rauch made a similar statement to ABC News last fall.

I met with Dr. Rauch in Cambridge, Mass., several years ago. He has read my “Wind Turbine Syndrome” book. You’re welcome to contact him for his clinical opinion. Notice, he actually treats WTS victims, and furthermore his specialty is neuro-otology — precisely the clinical specialty appropriate to WTS, since WTS is mainly a vestibular disorder. (You might consider Dr. Rauch the “pope” of vestibular disease.)
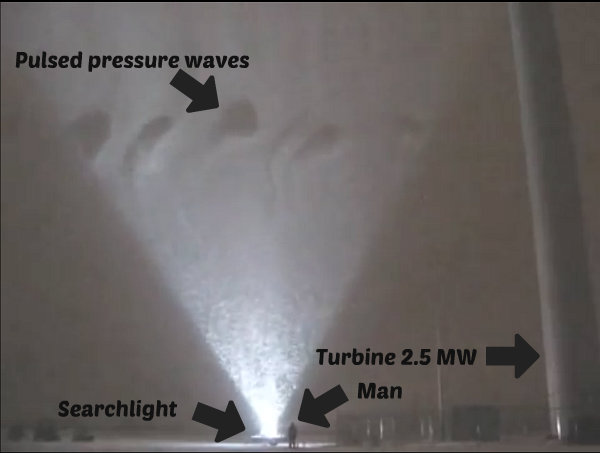
Shifting gears, a group of mechanical engineers at the University of Minnesota recently mapped the airflow turbulence patterns of a 2.5 MW wind turbine. Their technique was ingenious: “A large searchlight with custom reflecting optics generated a two-dimensional light sheet next to the 130-m-tall wind turbine for illuminating the snow particles in a 36-m-wide by 36-m-high area.” They literally mapped the vortices being hurled off the turbine blades, using a blizzard (!) as a kind of background screen.
Visit this website to see and savor the dramatic results.
Click open the video and notice the pulsed pressure waves from the blades — punching holes, as it were, in the swirling snow. (You can also watch the video on YouTube. That is, until the wind energy lobby manages to get it taken down.)
Think of volleys of acoustic artillery, much of it in the low frequency and infrasound range. Imagine the residents of Cesme being bombarded by this day and night.
You are looking at the huge, pulsed, sound pressure waves responsible for Wind Turbine Syndrome. (The Minnesota group published their article: Jiarong Hong et al., “Natural Snowfall Reveals Large-Scale Flow Structures in the Wake of a 2.5-MW Wind Turbine,” Nature Communications, vol. 5, no. 4216 (June 2014).
Ms. Kura tells me the turbines destined for Cesme are 3 MW. Several years ago, the noted Danish noise engineer, Professor Henrik Moller at Aalborg University, published a paper titled “Low-Frequency Noise from Large Wind Turbines,” Journal of the Acoustical Society of America, vol. 129, no. 6 (June 2011), pp. 3727-3744. Moller and his colleague, Christian Sejer Pedersen, demonstrated that “the larger the turbine, the greater the ILFN (infrasound and low frequency noise) produced.” The following is the abstract of their paper. (Professor Moller was summarily fired this spring. Click here for the story, which has the wind industry’s fingerprints all over it.)
As wind turbines get larger, worries have emerged that the turbine noise would move down in frequency and that the low-frequency noise would cause annoyance for the neighbors. The noise emission from 48 wind turbines with nominal electric power up to 3.6 MW is analyzed and discussed.
The relative amount of low-frequency noise is higher for large turbines (2.3–3.6 MW) than for small turbines (2 MW), and the difference is statistically significant. The difference can also be expressed as a downward shift of the spectrum of approximately one-third of an octave.
A further shift of similar size is suggested for future turbines in the 10 MW range.
Due to the air absorption, the higher low-frequency content becomes even more pronounced when sound pressure levels in relevant neighbor distances are considered.
Even when A-weighted levels are considered, a substantial part of the noise is at low frequencies and, for several of the investigated large turbines, the one-third octave band with the highest level is at or below 250 Hz.
It is thus beyond any doubt that the low-frequency part of the spectrum plays an important role in the noise at the neighbors.
Given all of the above, you can see why I am concerned for the residents of Cesme.
A final word. The clinical literature, including publications by the World Health Organization on health effects from infrasound exposure, typically use the word that Dr. Kelley used in his reports to the US Department of Energy — “annoyance.” It’s really not an appropriate word. It vastly understates the sickness caused by infrasound exposure. (A mosquito bite is an annoyance. Wind turbine infrasound, on the other hand, triggers a debilitating cascade of illnesses whose features I enumerated, above.)
In medicine, we clinicians are morally bound to exercise what’s called the “precautionary principle.” That is, if we don’t know for certain that a procedure is harmless, we are obliged to exercise extreme caution in performing the procedure, in this instance building industrial wind turbines — which are well-known to produce impulsive (i.e., amplitude-modulated) infrasound — near people’s homes. This is, after all, common sense.
For decades, the wind industry flatly denied their turbines produced infrasound. It took monumental efforts by people like me to debunk this fallacy. Wind industry advocates likewise argued that only downwind turbines created noise, that is, low-frequency noise. Dr. Kelley and his research team effectively debunked that falsehood, in the articles referred to above. Finally, the wind industry clung to the fiction that, “If you can’t hear it, it can’t hurt you.” Professor Salt deflated that one.
It’s time to recognize that the global wind industry has hidden behind a series of (what turned out to be) falsehoods. Their untruths have been exposed and corrected in the published clinical and scientific literature, as shown above.
There is no excuse for building wind turbines in proximity to people’s homes.
Comment by Helena Greenberg on 07/03/2014 at 3:15 am
Welcome to Green Hell!
“Tortured by the thousand through sleep deprivation, rural families are the collateral damage of this new regime whose war is against common sense and moderation. Their concentration camps are their own homes: moving isn’t affordable if one’s house loses a big chunk of its value and one’s income is tied to the location.”
Read more here.
Comment by Itasca Small on 07/03/2014 at 9:00 am
Once again, Dr. Pierpont has done an exceptional job in warning the wisely concerned residents of Cesme, Turkey, with valuable facts that should alarm everyone in their community, and everyone anywhere in the world who has the opportunity to read her letter. The links within the body of the letter are well-worth following for those who want to learn the truth about Industrial Wind Energy.
The video of infrasonic vortices created by IWTs in a blizzard is a one-minute “picture worth a thousand words!”
The excerpt from Professor Salt and Professor Lichtenhan’s paper includes the following:
“No one has ever evaluated whether tympanostomy tubes alleviate the symptoms of those living near wind turbines. From the patient’s perspective, this may be preferable to moving out of their homes or using medical treatments for vertigo, nausea, and/or sleep disturbance. The results of such treatment, whether positive, negative, would likely have considerable scientific influence on the wind turbine noise debate….”
I’m sure they mean well, but, are they suggesting that a procedure intended to be temporary, albeit over six months or so, might be an acceptable alternative?
WE ARE THE VICTIMS HERE!
Why should we be the ones to even consider surgery when we’re not the criminals causing the problem?
The wind industry has known that their monstrous machinery causes adverse health effects since at least the 1980s. Now, these professors seriously consider the possibility that we could be forced to resort to repeated temporary, otherwise unnecessary, surgeries on the unlikely chance that we could stay in our homes to continue being subjected to this MAN-CAUSED DESTRUCTION!!!
We’re already lab rats and guinea pigs to mad pseudo-scientists, businessmen, government officials/agents, etc., who have NO concern, sympathy, empathy, nor compassion for THEIR VICTIMS!
Why on God’s Green Earth should we have to even think that we might have to resort to “such treatment?”
The industry knows full-well what they are doing to us. I believe they take sadistic pleasure in the power-trip it gives them, knowing they are torturing untold numbers of humans and animals with 21st Century versions of the “rack” — and getting paid handsomely to do it!
Ahh, but, whether the surgery proved positive or negative, the scientific influence upon the debate would be considerable! And the rats and guinea pigs will either feel better and live longer, or feel no different and die sooner. Yes, but, the debate would be considerably “influenced!” Researchers would have new fodder with which to experiment for the next few decades while we suffer and die. . . .
[Hmm, I guess such surgery could create a lucrative market for ear-surgeons and their entourages — if it worked — considering all the people who will eventually be needing relief as long as the IWTs keep-on turning across-the-globe. . . . Even the veterinarians could jump on the bandwagon and insert tubes in their patients’ eardrums!]
No human being should ever be asked to allow “Band-Aid” surgical procedures in his ears, just because he can’t or won’t move away from the MAN-MADE CAUSE OF HIS AFFLICTION.
WE’RE NOT THE ONES WHO NEED TO MOVE!!!
WE ARE ALREADY VICTIMS OF AN UNSPEAKABLE CRIME!!!
WE SHOULDN’T BE FORCED TO MOVE OR SUFFER AND DIE!!!
AND WE DON’T NEED DR. FRANKENSTEIN EXPERIMENTING IN OUR EARS!!!
Dr. Kelley, et.al., found: “Further, there is evidence that the strong resonances found in the acoustic pressure field within rooms [in people’s homes] . . . indicates a coupling of sub-audible energy [infrasound] to human body resonances at 5, 12, and 17-25 Hz, resulting in a sensation of whole-body vibration (p. 120).” And, Dr. Pierpont’s study independently showed: “I discovered the same thing in my research. What Kelley refers to as a ‘sensation of whole-body vibration,’ I refer to as Visceral Vibratory Vestibular Disturbance (VVVD): . . .”
I would really like to know if the entire cascade of adverse effects to my body that nearly killed my adrenal glands, and by extension, my life, were all caused by the vestibular effect. (Along with being in all of Dr. Pierpont’s risk factor classes, I am one of those who could perceive infrasonic waves when they passed through my body unimpeded even before the IWTs invaded.)
It would be extremely helpful to know if anyone is known to have non-functioning vestibular organs. If so, is he physically affected by infrasound? Because, I believe the infrasound that can so drastically agitate the inner ear must also directly affect the other cells and organs in the body through the “. . . coupling of sub-audible energy [infrasound] to human body resonances . . .”
If the infrasound is coupled to human body resonances outside the Inner Ear, the overall effect is a combination of vestibular effects and the direct vibratory effects on other organs and cells at the same time. If the vestibular organs were non-functioning, it seems that symptomatology would occur but be somewhat different — as was mine with already weak adrenals. If this is true, then, tympanostomy tubes might reduce the adverse effects, but not “Band-Aid” the WTS in a meaningful way. Stressing the other organs and cells would still cause bad effects and overdrive/destroy the adrenals. (If I’ve forgotten something from Dr. Pierpont’s book, I apologize — my memory has not fully recovered from the effects of the infrasound.)
Nikola Tesla studied infrasound extensively and concluded that it is destructive to living cells. This was a monumental discovery, and now, decades later, it should be considered along with the ESSENTIAL discovery by Dr. Pierpont that the inner ear, and its influence, is significantly impacted by wind turbine infrasound. The proof is blatantly evident that Wind Turbine Syndrome is real. The only reasons the turbines still turn and we continue to suffer, are the evil ulterior motives of the perpetrators, and the indoctrination of the masses.
Further, Dr. Pierpont says: “Wind industry advocates likewise argued that only downwind turbines created noise, that is, low-frequency noise. Dr. Kelley and his research team effectively debunked that falsehood, . . .”
In 1987, Dr. Kelley, et.al., reported that: “low-frequency acoustical loads radiated from both individual turbines and groups of upwind and downwind turbines. . . .” I can attest to this fact in my own community’s experience. Our symptomatology increases and decreases as our predominantly SW winds — upwind to the turbines most of the time — shift through the compass directions, with the 2.2MW turbines northwesterly to southeasterly across the center of the circle. The worst times are when the wind is out of the NW. It is at least approximately 10.5 – 13 miles ENE to the nearest IWT.
Also, “Moller and his colleague, Christian Sejer Pedersen, demonstrated that ‘the larger the turbine, the ongreater the ILFN (infrasound and low frequency noise) produced.’ ” And, that: “The relative amount of low-frequency noise is higher for large turbines (2.3–3.6 MW) than for small turbines (2 MW), and the difference is statistically significant.”
If the difference between “low-frequency noise” of 2.3 – 3.6MW and 2.2MW turbines is statistically significant, and the 2.2MW turbines at least ~10.5-13 miles distant, forced me and others from our homes — and are adversely affecting others — then, just imagine how far and how seriously the larger ones will destroy lives!
Yes, Dr. Pierpont, the setbacks must be more than 2km; 5km is a start and may well be enough for now, in the particular conditions in Cesme. But, I will rejoice when more researchers believe there are those of us in different localities who are being victimized by IWTs at much greater distances. . . .
If the evidence in Dr. Pierpont’s letter does not convince the reader that there is something rotten in the wind industry, and in all the governmental, pseudo-scientific, and media support for it, NOTHING WILL.
Many people worldwide are like blind sheep, believing the lies out of ignorance and trust. However, if truth is presented and they still reject it, their willful blindness becomes guilt, as they aid and abet the crime.
The biggest truths about Industrial Wind Energy are:
THERE IS NO SAFE DISTANCE FOR WIND TURBINES ON PLANET EARTH!!!
WIND ENERGY WILL NEVER SAVE THE PLANET!!!
Itasca Small
Wind Energy Refugee
Comment by Katarina Dea Zetko on 07/03/2014 at 4:20 pm
Dear friends from Turkey,
I just want to say that we are on your side. Do not let this happen. Wind turbines are taking away the most important thing we have — our mental and physical health.
We are dealing with the same kind of problems, and dr. Nina Pierpont and her husband Calvin Luther Martin are always ready to help.
Do not forget, you are not alone in this terrible war; WW4 and Slovenia are with you.
Katarina
Comment by Curt Devlin on 07/04/2014 at 10:10 am
To Madeleine Kura, I can say with great sincerity, that I know and understand how you must feel. My own town is a naturally and architecturally beautiful place by the sea, just as Cesme is. Unfortunately, it lacked the economic and political power necessary to fend off the onslaught of wind developers in collusion with government officials.
I know firsthand the looming shadow of social injustice and turmoil cast by these destructive mechanical monsters as they approach. I’ve heard all the sickening lies, deceptions, and false promises of wind developers and their crony capitalist cohorts. It is easy to feel over-matched, but you must do all that you can to fight this while you still can.
Asking Dr. Pierpont for help was a very important first step. I did the same. Now it is your job to make sure that people in Cesme hear what she, and those she cites, have said. As Plato said, truth without power is impotent.
To Dr. Pierpont, I must say thank you once again for doing what you have done for Madeleine and Cesme, just as you did for me and Fairhaven. It is no small thing to lend what you have learned about illness and health, to those who need it most. If only all doctors took their responsibilities as seriously as you do.
As Martin Luther King once said, “Injustice anywhere is a threat to justice everywhere. We are caught in an inescapable network of mutuality, tied in a single garment of destiny. Whatever affects one directly, affects all indirectly.”